
Flu Prevention? Try Paid Sick Days
0 Comments
This is repost written by Ellen Bravo,
[caption id="attachment_5692" align="alignnone" width="570"] Source:Huffington Post (AP

[caption id="attachment_5681" align="alignleft" width="140"] Robert Bollinger, MD,


Anger and shame: Irish women protest following the death of Savita Halappanavar Source: The Telegraph; Photo: AFP/Getty Images
I’m tempted to say that Savita Halappanavar died at University Hospital Galway in Ireland from a 17-week, wanted pregnancy that went awry. But it’s more accurate to say that she died in a Catholic country from a policy that deemed the heartbeat of a dying fetus to be more important than the life of its mother. Some may argue that Halappanavar would not have died had she been in a U.S. hospital, but after the wrangling over reproductive rights in the last year’s national elections I think she very well could have.
Halappanavar was 31 years old when she was admitted to University Hospital Galway for back pain. According to the Irish Times, she presented fully dilated and leaking amniotic fluid. When she was told that a miscarriage was in process, she requested that the pregnancy be terminated. But the fetus still had a heartbeat, her doctors said, which meant in that Catholic hospital and country that terminating the pregnancy was not permissible. It didn’t matter that she was not Catholic. Three days later, the fetus died and Savita Halappanavar was admitted to the intensive care unit, where she died of septicemia.
Abortion is illegal in Ireland, except to save the life of the mother. But, as noted in a 2010 report by Human Rights Watch, that country rarely supports this exception. Marianne Møllmann of Amnesty International maintains that health professionals in Ireland want clarity on when they can intervene in cases like Halappanavar’s without fear of criminal prosecution. Indeed, in the case of Halappanavar, the hospital and its clinicians essentially invoked a “conscience clause” that provides health care providers to opt out of intervening in ways that they find morally objectionable. Dr. Jen Gunter, an OB-GYN physician, has suggested that the clinicians didn’t intervene because they did not want to be judged as violating the country’s abortion laws and criminally prosecuted. She argues that Halappanavar’s symptoms should have assured that she receive pain medication and a termination of the pregnancy immediately to prevent sepsis.
Could this happen in the United States, where abortion is legal?


Source: Rainbow Babies and Children’s Hospital
When you think of newborns who are in a neonatal intensive care unit, you assume that the baby is receiving the best of evidence-based care. There has been a great deal of research on medical interventions for these distressed newborns, but not as much nursing research on some of the important routine care issues. And this situation could worsen, depending upon the upcoming budget negotiations between President Obama and Congress. Consider the example of how to feed distressed, very ill neonates.
Gail McCain, PhD, RN, FAAN, Dean of the Hunter-Bellevue School of Nursing, has been studying the feeding of neonates for over two decades. Her work has been instrumental in our understanding of the cues that distressed neonates demonstrate to show they’re hungry. These cues are seldom the same as “term infants” (fully developed and delivered at a minimum of 40 weeks of gestation), so nurses, physicians, and even parents may not recognize that the neonate is hungry and ready to feed.
In the December 2012 issue of Nursing Research, widely considered the gold standard for nursing research journals, McCain and her colleagues report on a randomized clinical trial that focused on preterm infants with bronchopulmonary dysplasia, a condition in which the neonate’s underdeveloped lungs are injured from being on a ventilator and oxygen therapy for treatment of another respiratory condition, acute respiratory distress syndrome. These very sick infants are usually given tube feedings instead of nipple feedings. Nipple feedings can cause more respiratory distress, as the infant has to work to suck and may not have the energy reserves and oxygenation capacity to manage this. So the standard approach to helping these infants to transition from tube to nipple is to limit the nipple feedings to predetermined times and frequencies. In this new study, McCain and colleagues tried a different approach based upon their prior research.
The researchers compared the standard treatment with an experimental treatment that they call the “semidemand” method. Semidemand is based upon assessing the infant for non-term cues, such as simply being awake or sucking on fingers, instead of crying, and watching them carefully as they feed to make sure they don’t get into physiological trouble while feeding (e.g. “infant initiated and sustained sucking without cardiorespiratory distress”). This approach required continual assessment of the infant by the nurse to determine if the infant was becoming distressed from the feeding. As the researchers note in their paper, this approach “allowed for feedings to be led by the infant, rather than by the nurse.”
It seems that every country is unsatisfied


Nancy Cabelus teaching sexual assault assessment class in Kenya
When the Government of Kenya passed the Sexual Offences Act of 2006, members of Parliament probably had no idea how important this landmark legislation was or how cumbersome it would be to sort out. The Sexual Offences Act (SOA) is a law that encompasses over 200 sex-related crimes ranging from gang rape to forced kissing. Prior to the passage of the SOA many of these crimes went without criminal investigation or punishment of the offender. An outcome of the SOA was the formation of a Sexual Offences Act Task Force, a multidisciplinary board chaired by a judge and comprised of representatives of government ministries and some members of civil society. When problems arise within the scope of the SOA it indeed takes a village to find solutions. Such issues are brought forward to the SOA Task Force.
Historically, a major problem with clinical, post rape care was that only one doctor in the country was authorized to conduct post rape examinations in Kenya. Survivors of violence would sometimes wait in queues for days to be seen by this doctor. This untimeliness would result in physical evidence being lost or destroyed and any bodily injuries would be healed before the patient was examined. Worse, the doctor was expected by law enforcement to determine whether a crime of rape or defilement had occurred. In reality, it is not the duty of a doctor to determine if a crime has happened. Rather, it is the duty of the police to investigate violations of the law. The Kenyan people have been misled for decades to believe that a doctor could formulate a “diagnosis” of rape while rape is not a medical diagnosis. Rape is a crime that warrants police investigation.
Jim Stubenrauch is a CHMP senior fellow and a co-founder of the program in Narrative Writing for Health Care Professionals. Follow him on Twitter: @jimstuben.
At a press conference on Wednesday afternoon, five days after the mass murder in the Sandy Hook Elementary School in Newtown, CT, President Obama announced the formation of a task force on gun control to be headed by Vice President Biden—and then for the next 22 minutes of a half-hour Q & A, he took questions from a roomful of White House correspondents—the crème de la crème of the Washington press corps—about the so-called fiscal cliff. (Here’s a video and here’s the official transcript.)
At the precise instant that the POTUS stood up before the world and spent some precious political capital in declaring that, at long last, some serious effort would be made to end decades of paralysis on gun control and that substantive changes might soon help prevent acts like Adam Lanza’s slaughter of defenseless schoolchildren and teachers, the AP’s chief White House correspondent, Ben Feller, and the Wall Street Journal’s Carol Lee, among others, took the opportunity to turn away from discussion of this critical issue and return to the topic that had so preoccupied the news media before last week’s mass murder. The questions that followed amounted to an obsessively detailed but redundant parsing of the stalled budget negotiations. Half of that conversation is already old news.
I understand that this kind of thing happens all the time at presidential pressers, but in this particular instance I found the business-as-usual approach to the business of Washington insufferable and inappropriate. What this says to me—and I’m not the only one criticizing the press for this—is that the professionals in the room didn’t necessarily see the president’s statement as anything out of the ordinary; to them it was nothing more than the expected response to yet another routine tragedy that, in the long run, won’t make any difference in how guns are manufactured and sold, used and misused, or how—all too often in our country—innocent people die. The gun violence task force and the prospect of bipartisan support for gun control legislation are apparently of less moment than the same old same old about tax hikes and entitlement cuts. (And let’s leave aside the question of whether it’s accurate to say that we’re experiencing a “fiscal crisis” or whether what we’re hearing is anything more than the cynical maneuvering of antigovernment ideologues on behalf of the richest of the rich.)
Perhaps I found this incident particularly galling because of the way television and radio had been for the previous five days not only reporting on the shootings but dramatizing the nation’s collective response to the event.
[caption id="attachment_5611" align="alignleft" width="183"] Steve Gorelick[/caption] Media coverage
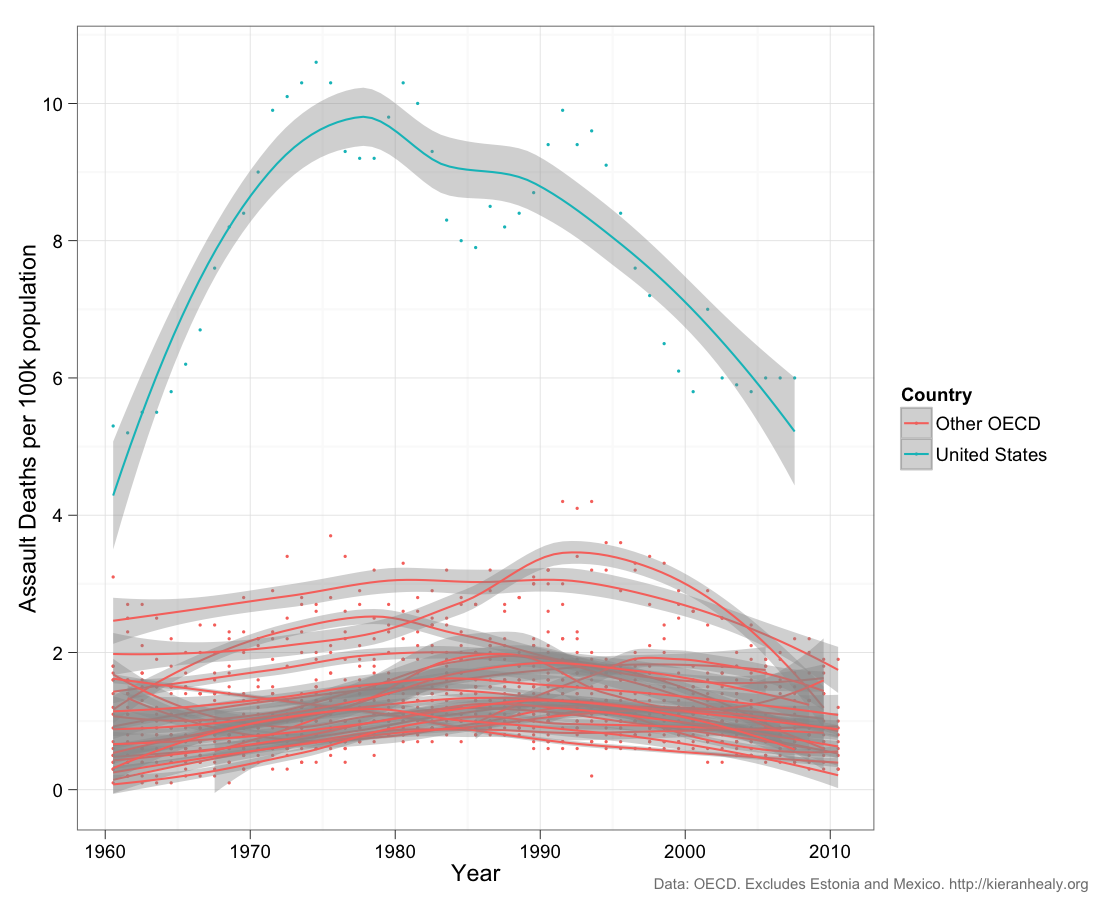
[caption id="attachment_5590" align="alignnone" width="1024"] Keiran Healy, Duke

